Please click this link for pre-test.請點選此連結進行前測
Chief complaint
Multiple joints painful swelling for weeks
Present illness
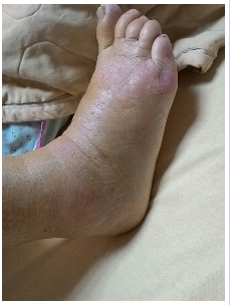
Mrs. Huang is a 78-year-old female patient with untreated hypertension and type 2 diabetes mellitus. She suffered from acute onset polyarticular pain with intermittent fever up to 38.3℃ 4 weeks ago. The joint involvement included bilateral shoulders and right elbows, right wrist, right 2nd and 3rd MCPs, bilateral knees, right dorsal foot and left 1st MTP. She mentioned that she injured her right elbow and ankle several months ago during a falling accident without evidence of fracture at the time. Due to fever and multiple joint painful swelling, she had visited local hospitals and was treated as gout and cellulitis respectively but the joint pain improved partially with rapid recurrence of both fever and joint pain. Upon admission, physical examination showed swelling with local heat of multiple joints especially at right knee, right ankle, right wrist and right MCP2/3, also with limitation of passive and active ROM noticed at bilateral shoulders, knees, right elbows, wrist and ankle. (Picture 1)
Picture 1 Right ankle
 Past history
Past history
hypertension
type 2 diabetes mellitus.
Personal History
Smoking: Nil
Alcohol: Nil
Betel nut: Nil
Travel history
No
Family history
Significant disease history in the family: Nil
Contact History
No
Laboratory Data
Blood test showed : WBC:8740 μL, Hb: 10.0 g/dL, PLT: 338 x 10^3/μL, Neut/Lym:84%/10.3%, hsCRP: 27.411 (< 0.3 mg/Dl), ESR: 115 (0-20 MM/HR), Uric acid: 2.4 (F:2.5-6.3 mg/dL), Ferritinl: 703.16 (4.63-204.0 ng/Ml), ANA: Equivocal 1:80, AC-4_Nuclear fine speckled. RF: negative. Anti-CCP: negative. Anti-SSA/SSB: negative.
Images
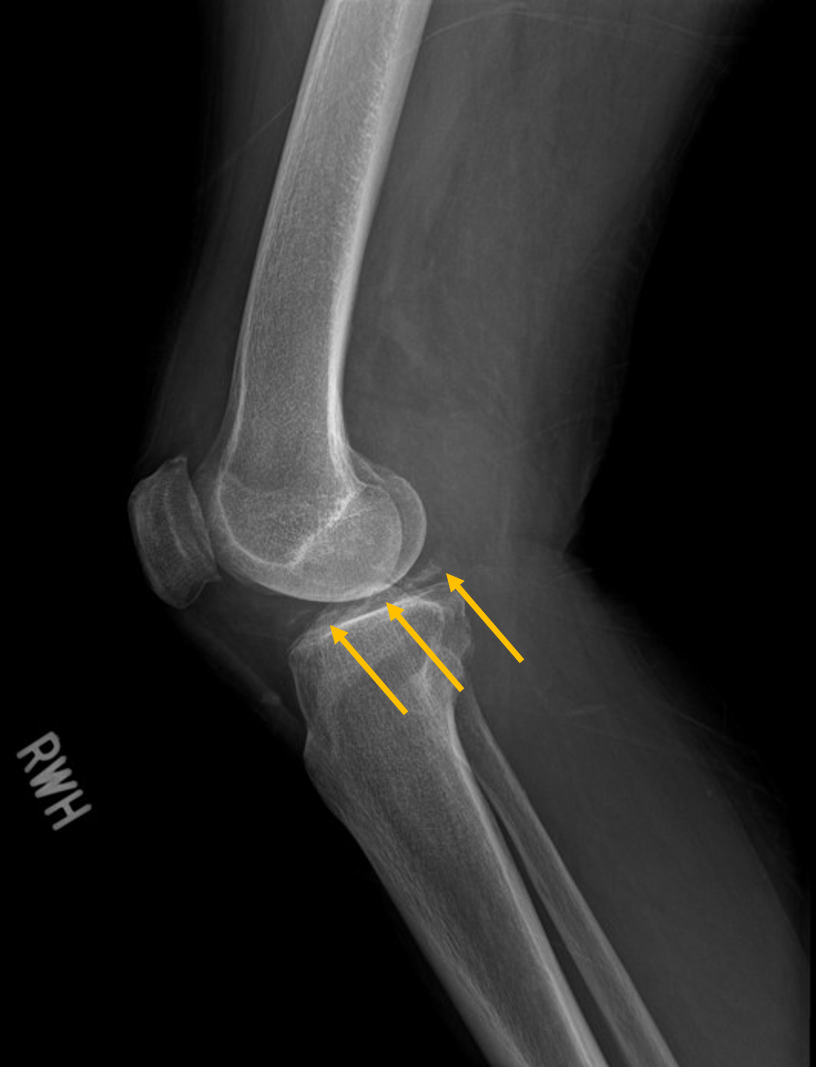
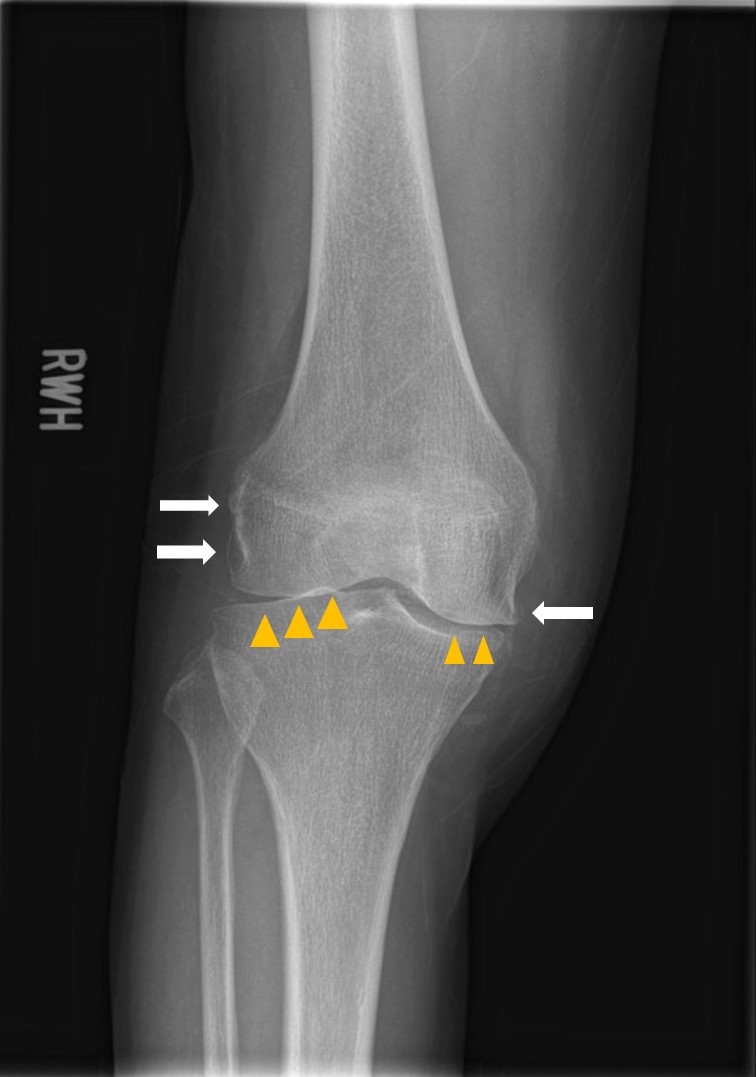
X ray image showed chondrocalcinosis over triangular fibrocartilage complex (TFCC) of right wirst (yellow arrow in Picture 2) and right knee (Picture 3). Asymmetrical joint space narrowing with spur formation (white arrow in Picture 4) of right knee was seen, compatible with OA change. No fracture or joint erosion seen over right elbow. (Picture 5).
Picture 2 Right Wrist
 Picture3 Right Knee Lat. view
Picture3 Right Knee Lat. view
Picture 4 Right Knee AP view
Picutre 5 Right elbow
 Ultrasonography
Ultrasonography
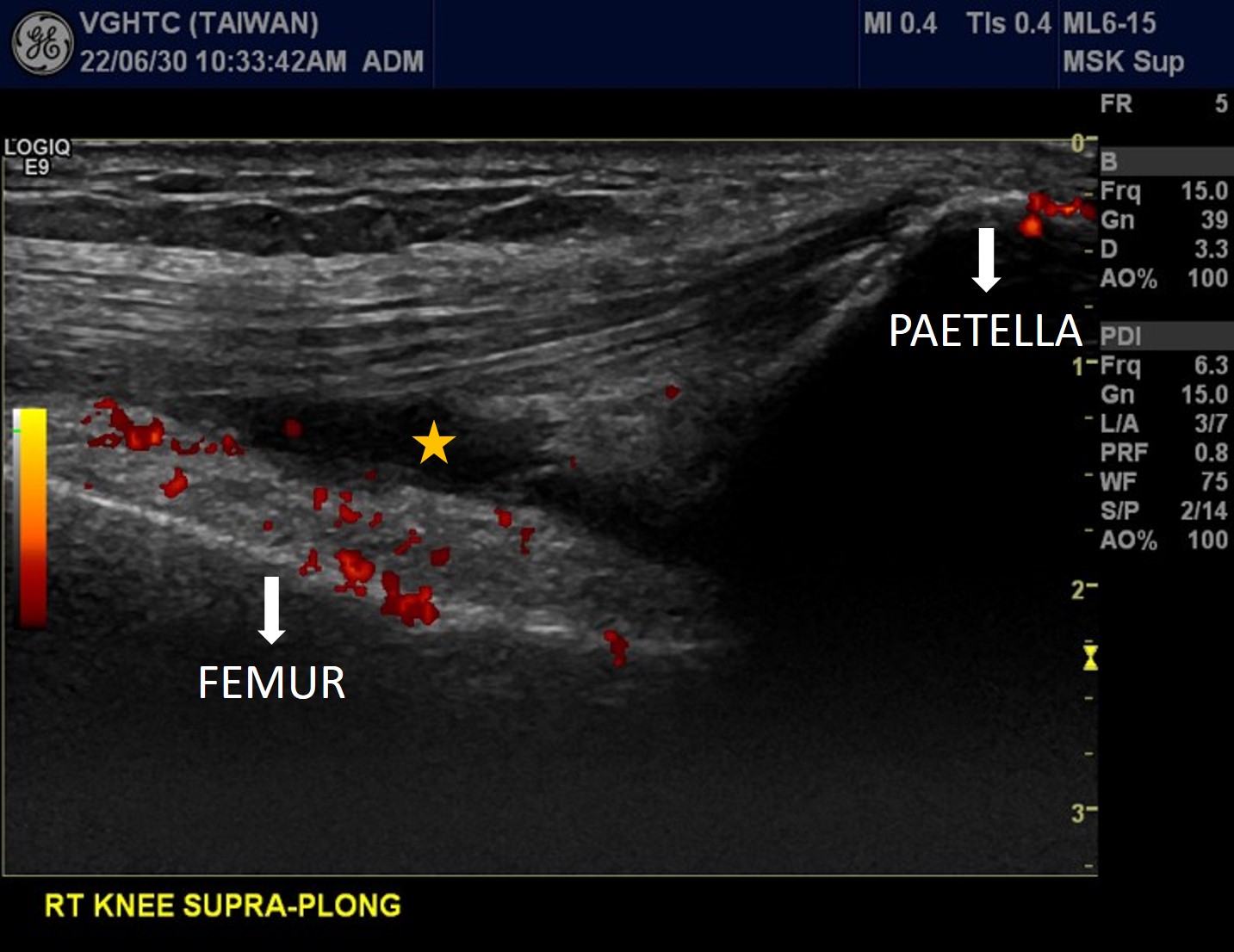
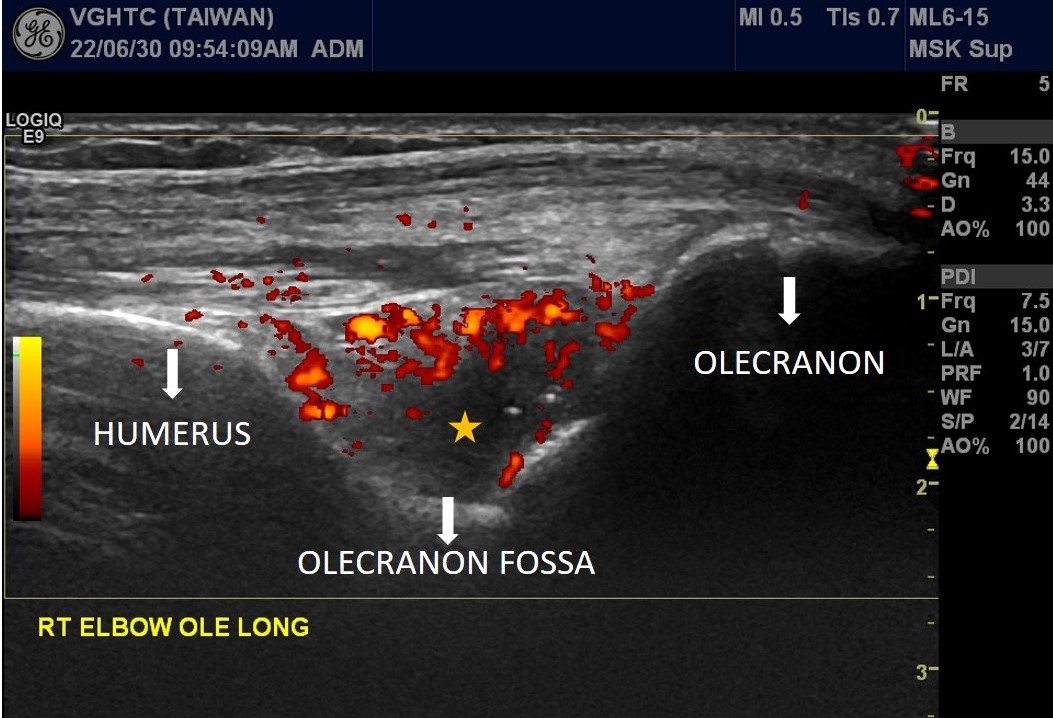
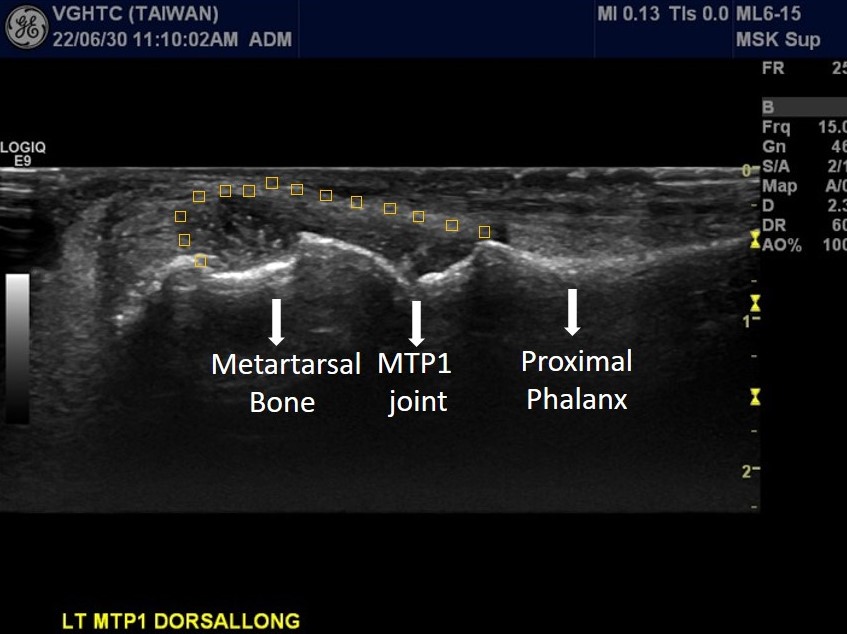
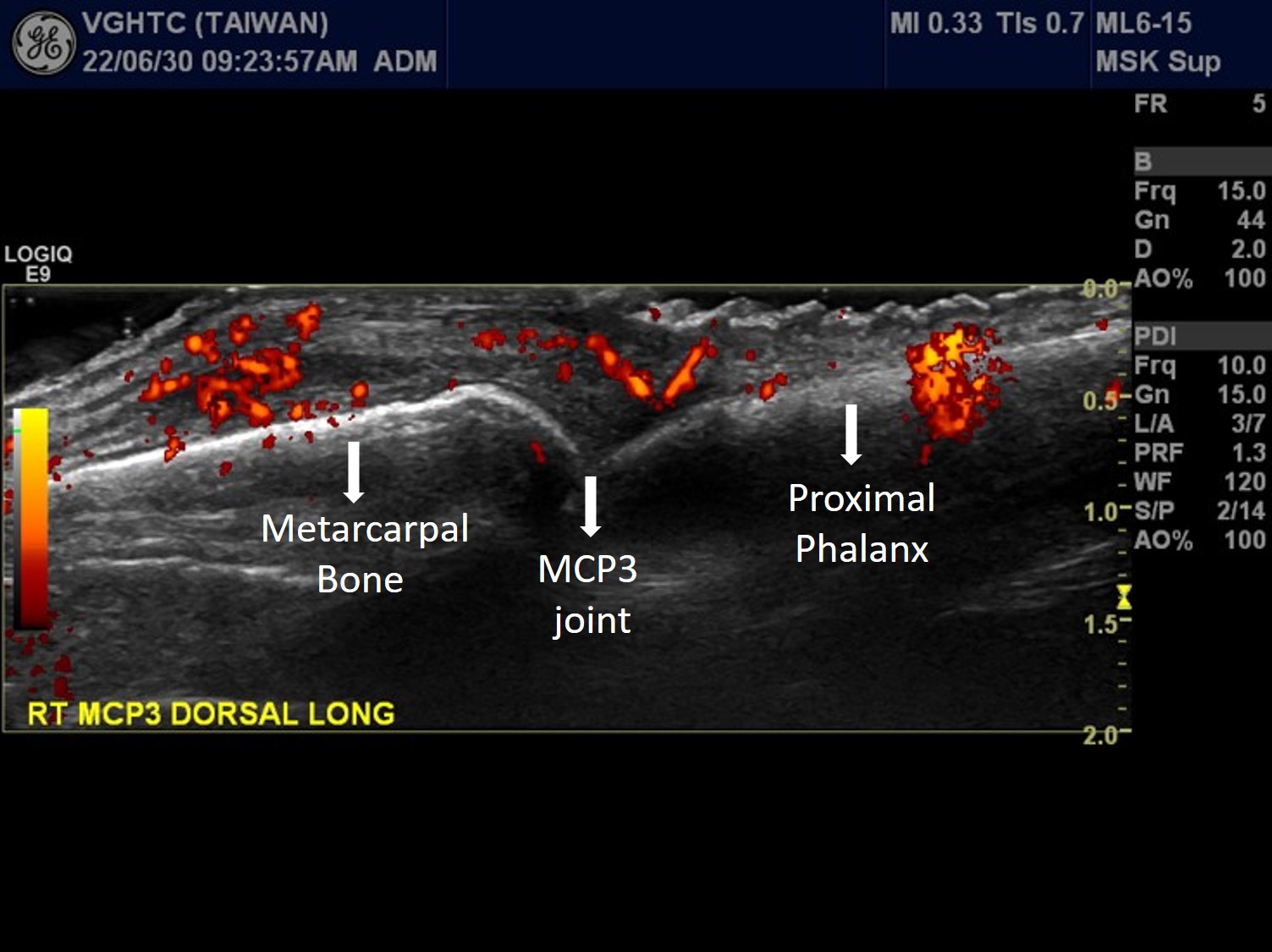
Longitudinal scan at suprapetellar region of right knee with power Doppler ultrasound showed increased joint effusion (asterisks in Picuture 6 ). Posterior longitudinal scan of right elbow with power Doppler ultrasound showed increased joint effusion at olecranon fossa (asterisks in Picutre 7) with hypervascularity (red color signal), indicating active arthritis of right elbow. Dorsal longitudinal scan at left MTP1 showed synovial hypertrophy with heterogeneous echogenicity , possible crystal deposition. (Picuture 8). Dorsal longitudinal scan with power Doppler ultrasound at right MCP3 showed synovial hypertrophy with hypervascularity (red color signal in Picture 9), indicating active arthritis.
Picuture 6. Rt Knee
Picuture7. Olecranon fossa of Rt Elbow
Picuture8. Lt MTP1
Picuture9. Rt MCP3
 Synovial Fluid Analysis
Synovial Fluid Analysis
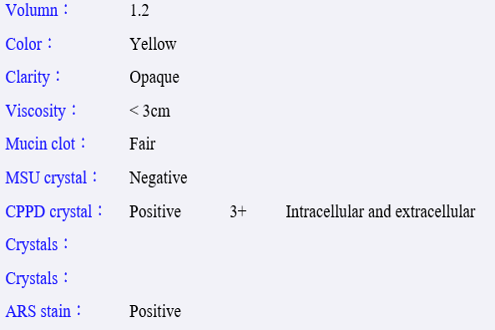
Aspiration of 7 cc yellowish joint effusion from both knees. (Picuture10) Joint fluid analysis showed WBC:12737(R) /1038 (L). (Picuture11) Inflammatory arthritis was considered. Polarizing light microscopy showed positive calcium pyrophosphate (CPP) crystal (Picuture12&13), both intracellular and extracellular.
Picuture10. Joint effusion

Picuture11. Joint Effusion analysis

Picture 12 Joint Effusion analysis-2
Picuture13. Polarizing light microscopy

 2022/9/7 11:57:07
2022/9/7 11:57:07
 979
979


