Hospitalization and diagnosis
Enoxaparin was administered initially for DVT but held for procedure and was not added back due to no clinical symptom/sign. Duodenoscopy was arranged on 2022/08/02 which showed reflux esophagitis, LA, Gr A; antral gastritis and ulcers; gastric polyp, high body; bile reflux with pathology showing chronic gastritis.
Echocardiography, abdominal sonography showed no significant findings.
For bilinear cytopenia(anemia, thrombocytopenia), mononucleosis, we had lab showing A/G reverse, elevated beta2-microglobulin, atypical; otherwise infection, metabolism less likely [EBV, CMV, HBV, HCV: WNL; thyroid, adrenal/Fe/vit B12/folate: WNL].
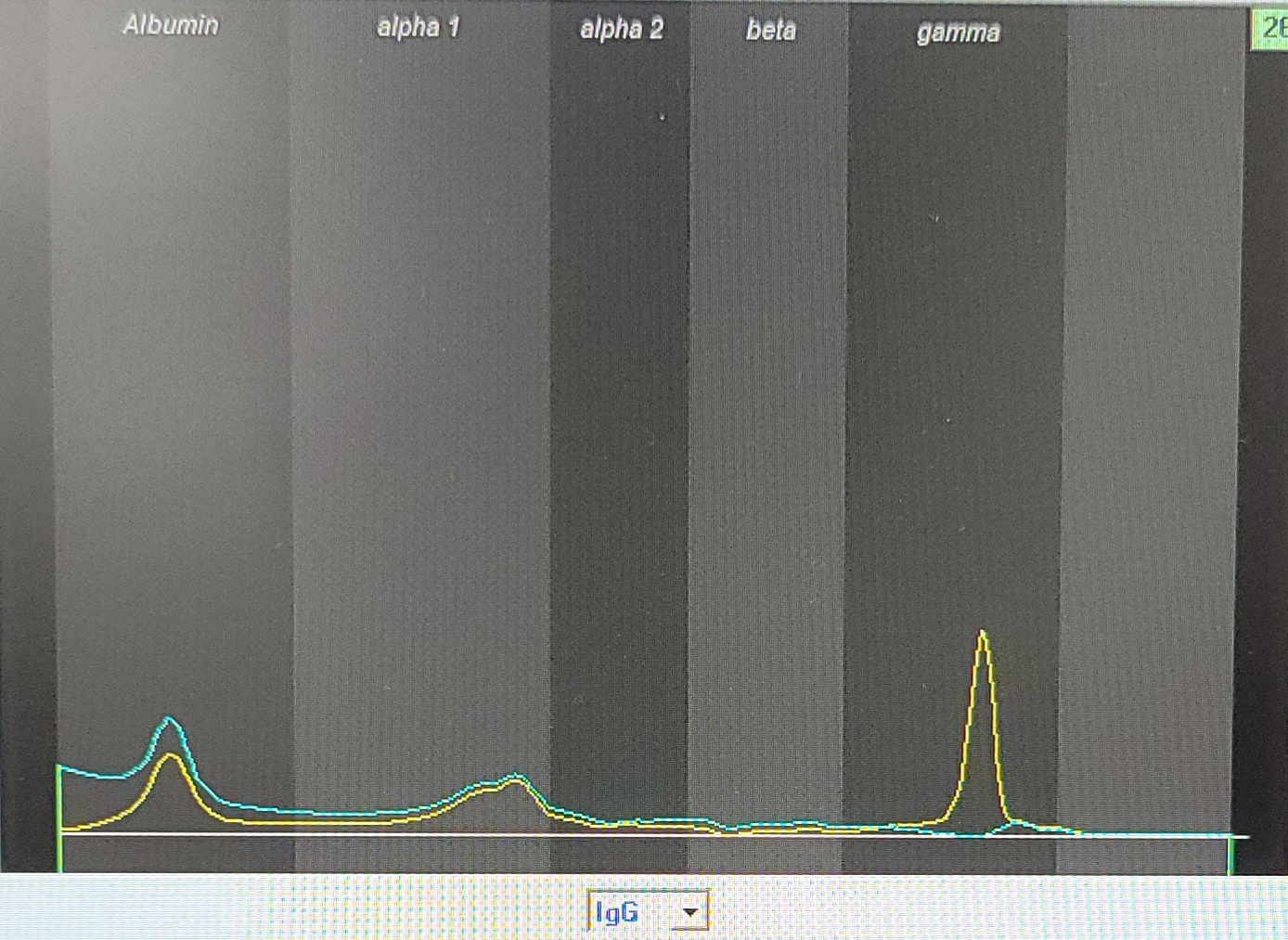
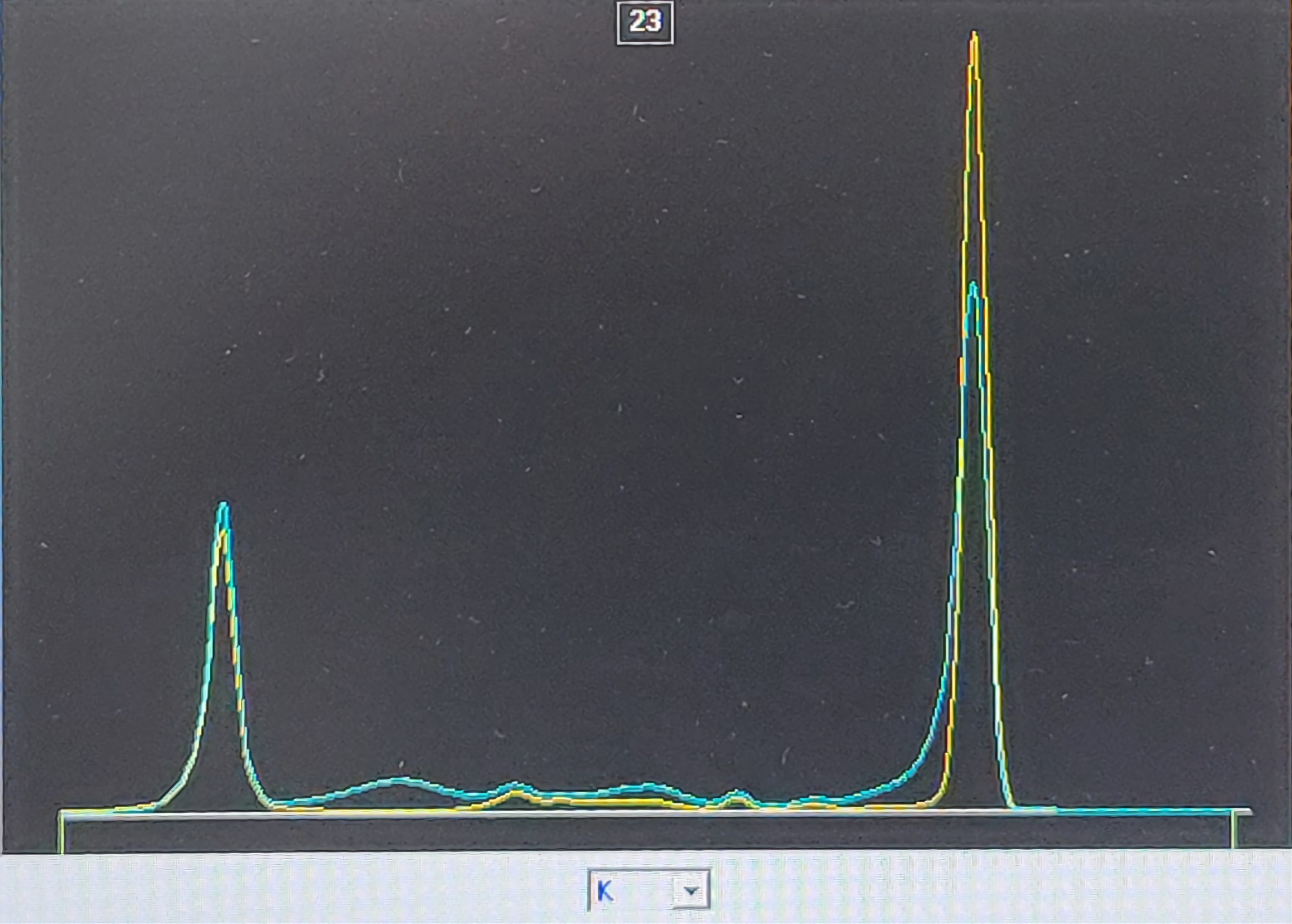
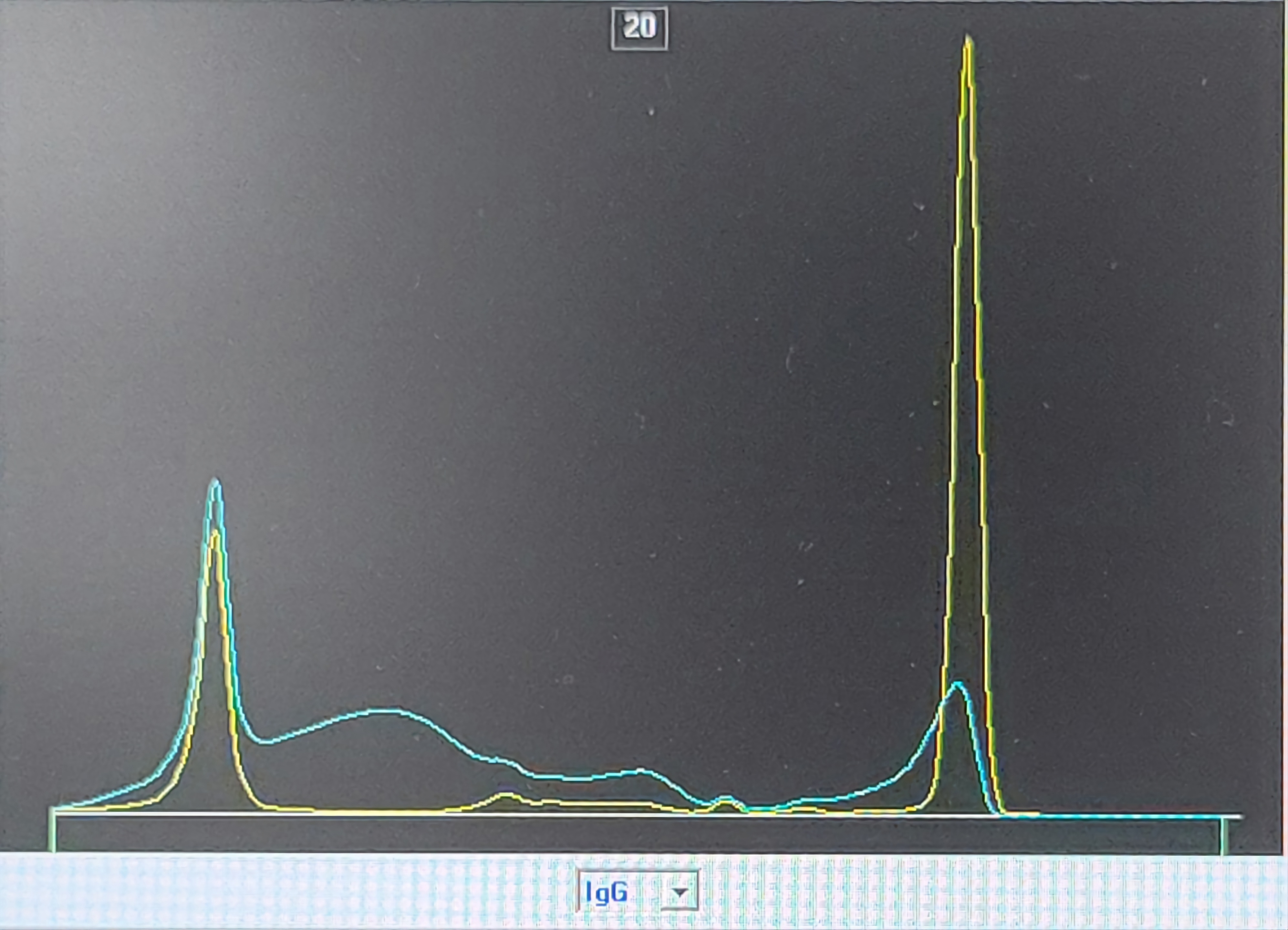
We then arranged serum and urine immunofixationelectrophoresis (IFE), which showed IgG/kappa monoclonal band(Picture 3 & Picture 4) and Hematologist was consulted with bone marrow biopsy showing plasma cell myeloma(Picture 5).
After empirical antibiotics and diuretic treatment, patient’s pleural effusion and dyspnea subsided. The patient was then discharged and HEMA OPD was arranged for further myeloma treatment.
Urine IFE showed IgG/Kappa monoclonal band(Picture 3).
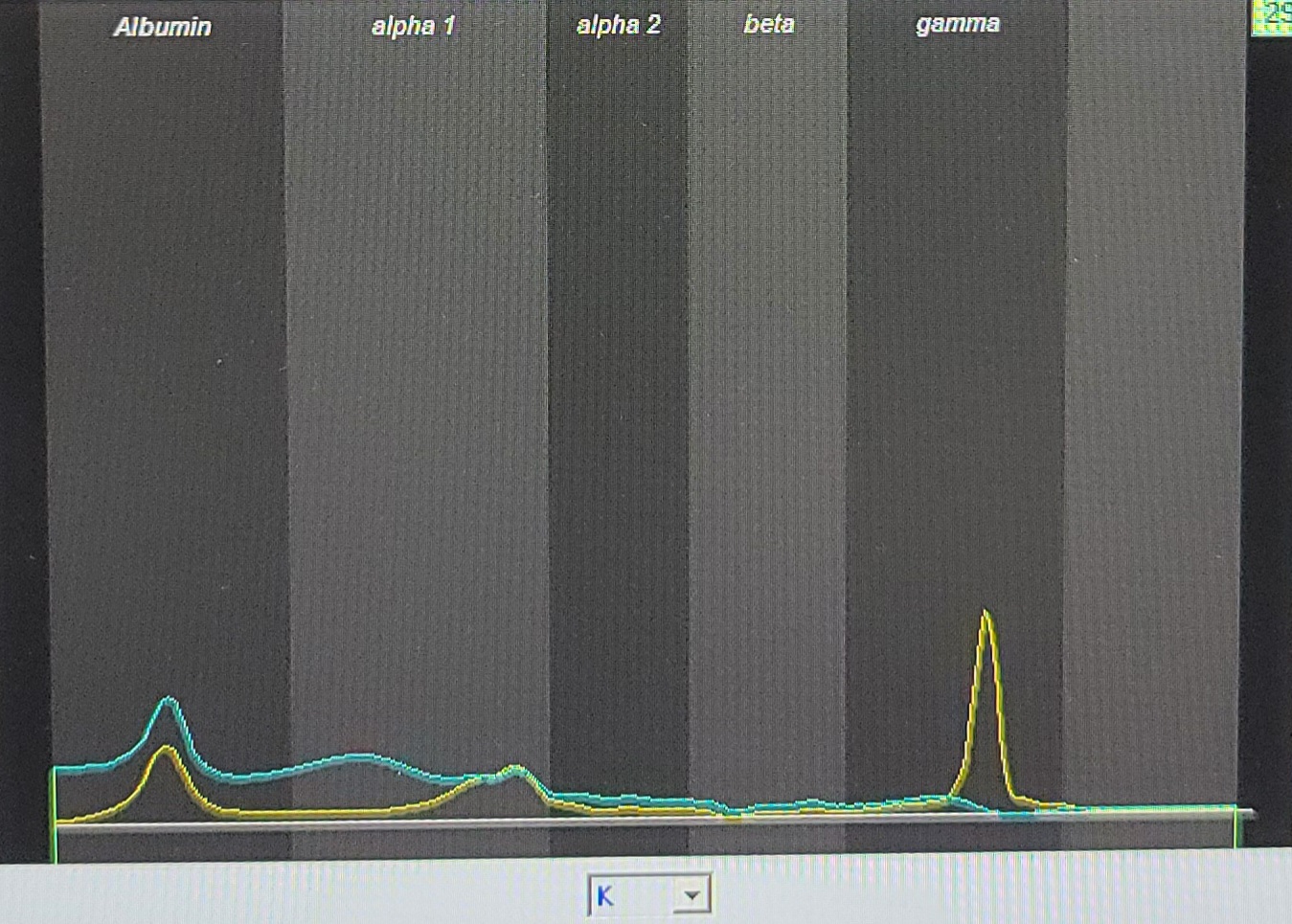
Serum IFE showed IgG/Kappa monoclonal band(Picture 4).
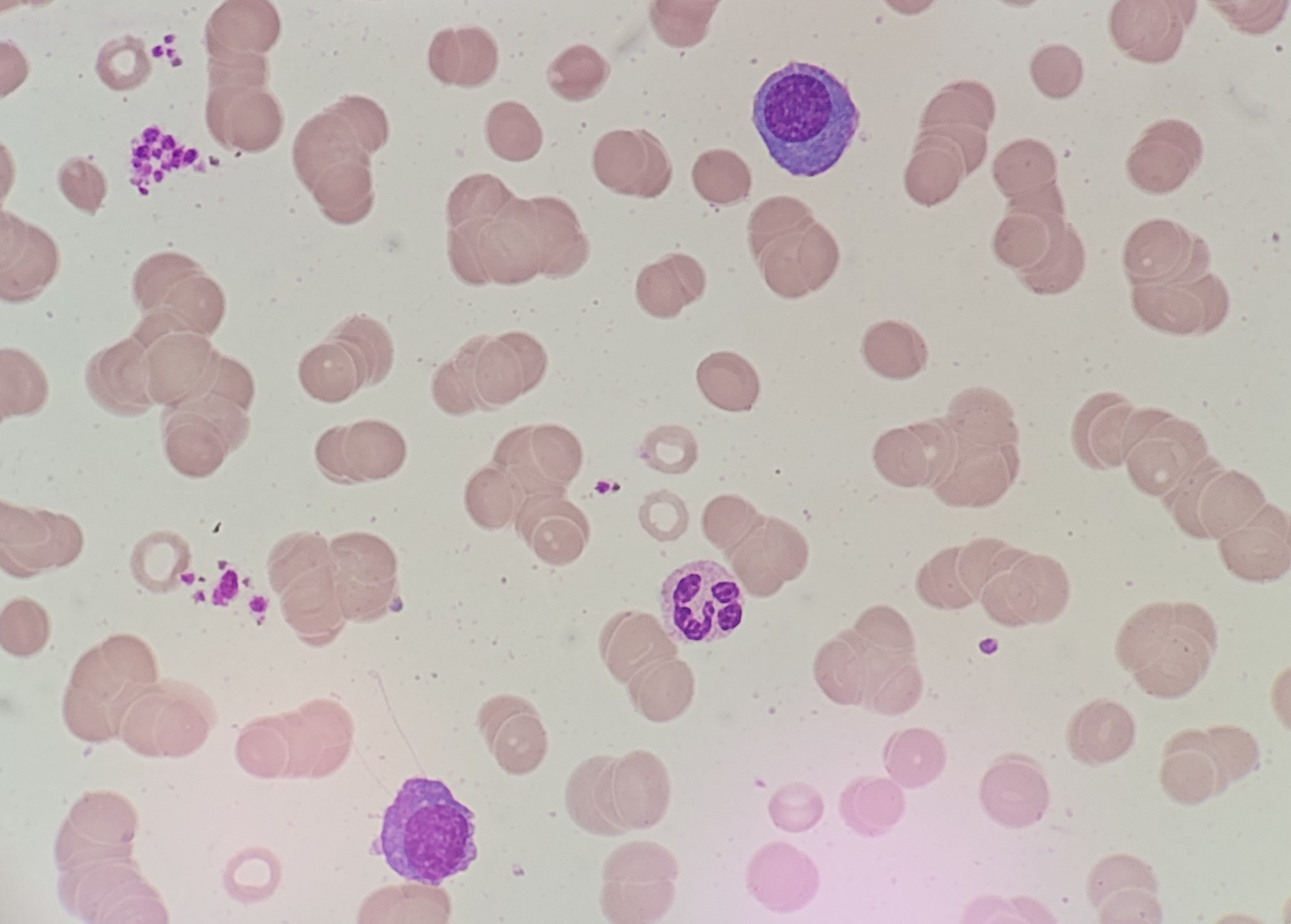
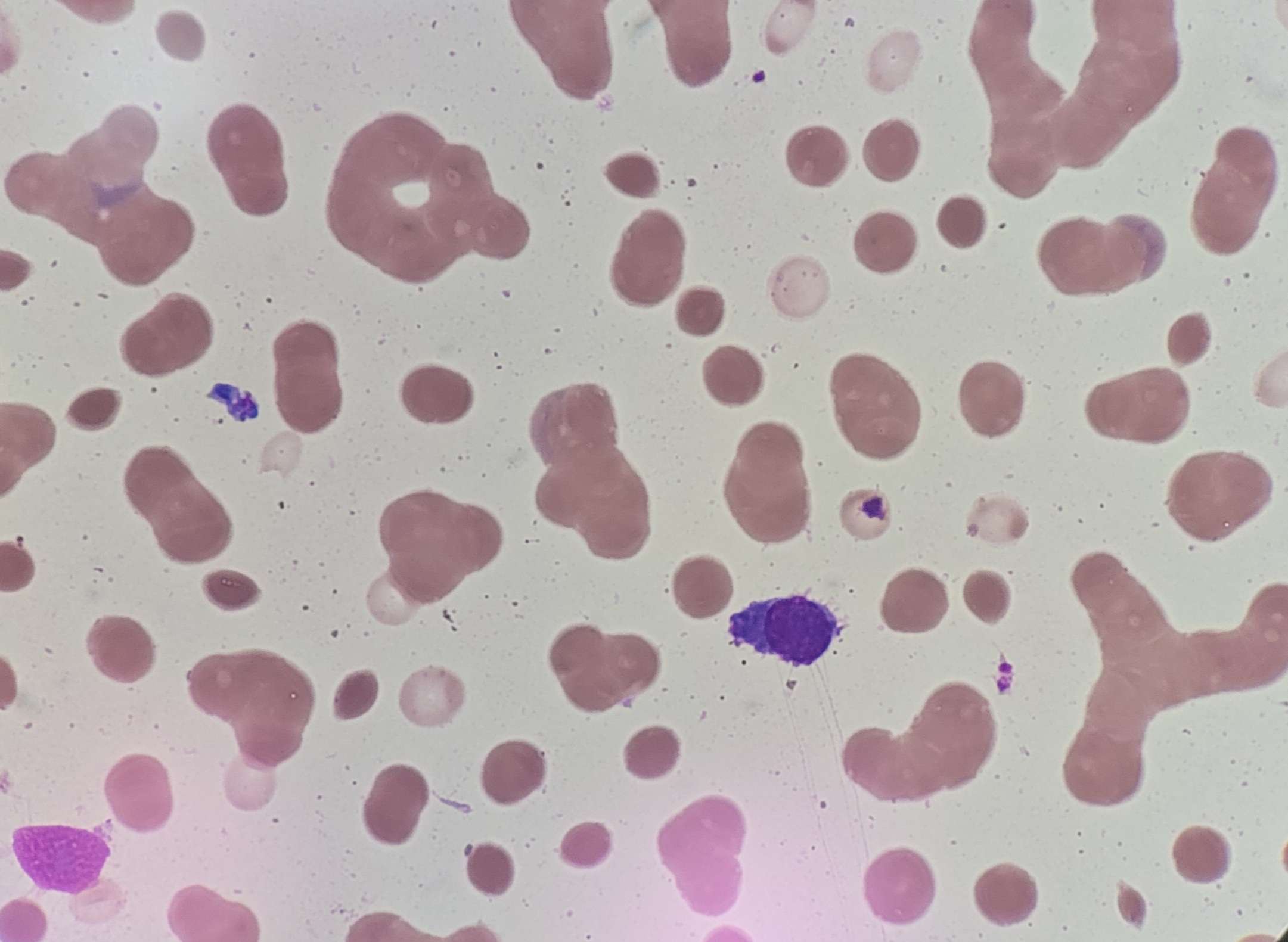
Bone marrow cytology showed atypical plasma cells and atypical lymphocytes, compatible with plasma cell myeloma(Picture 5).
 2022/9/6 8:07:52
2022/9/6 8:07:52
 967
967


