


Nelson Chapter 497 Medulloblastoma
引用 (4)
 2020/4/8 10:45:49
2020/4/8 10:45:49
 1764
1764
Nelson Chapter 497
Brain Tumors inChildhood by Joann L. Ater and John F. Kuttesch Jr.
Medulloblastoma VGHTC PED 20180102
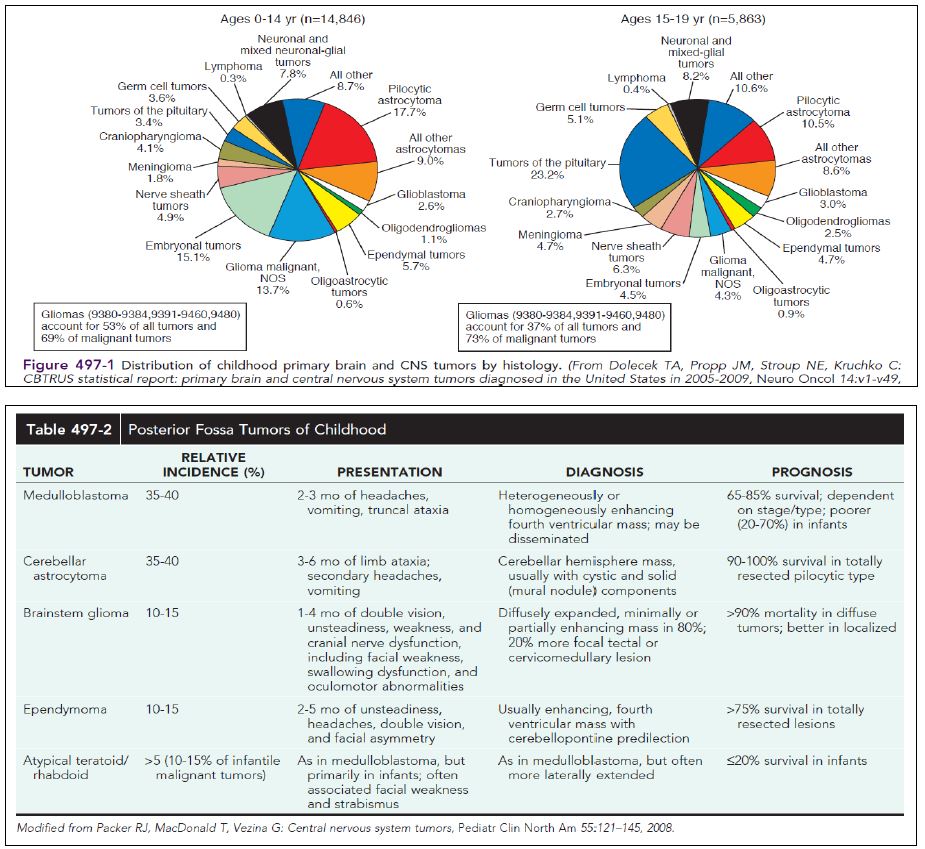
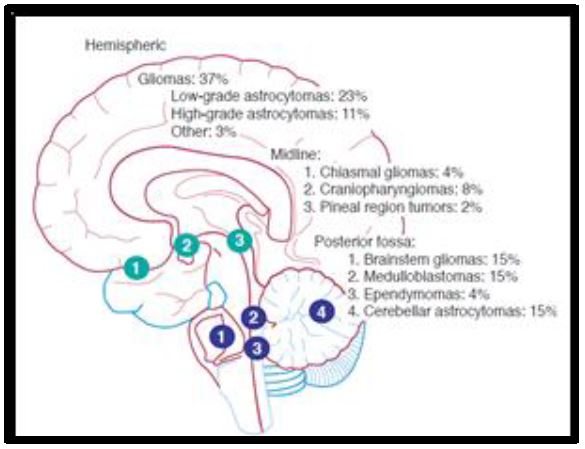
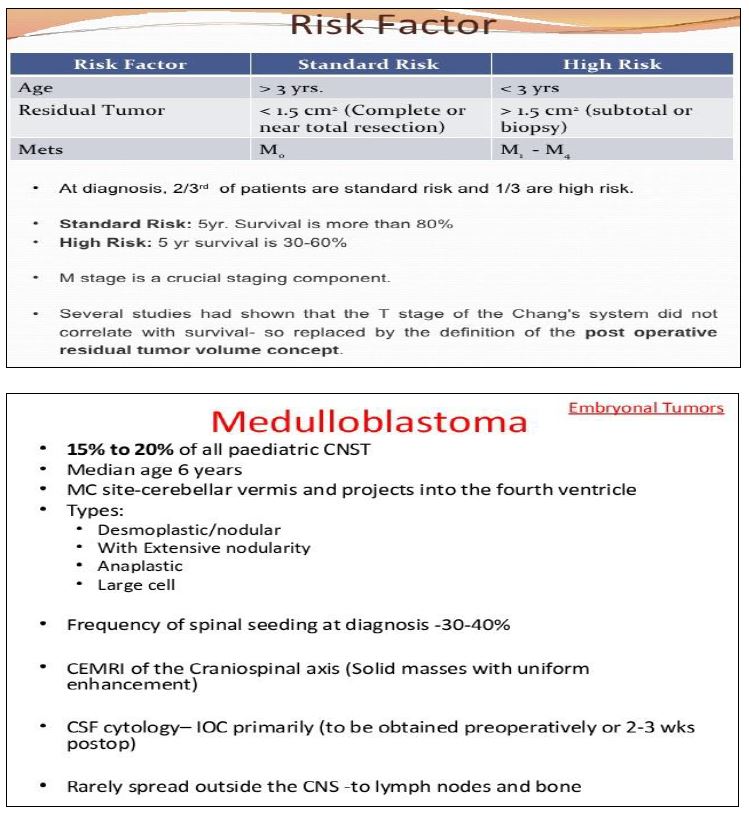
1. 90% of embryonal CNStumors; a cerebellar tumor; predominantly in males; median age of 5-7 yr。Location: in the midlinecerebellar vermis; older patients may inthe cerebellar hemisphere.
2. CT and MRI: a solid, homogeneous,contrast medium–enhancing mass in the posterior fossa causingfourth ventricular obstruction and hydrocephalus; up to 30% of patients with evidenceof leptomeningeal spread.
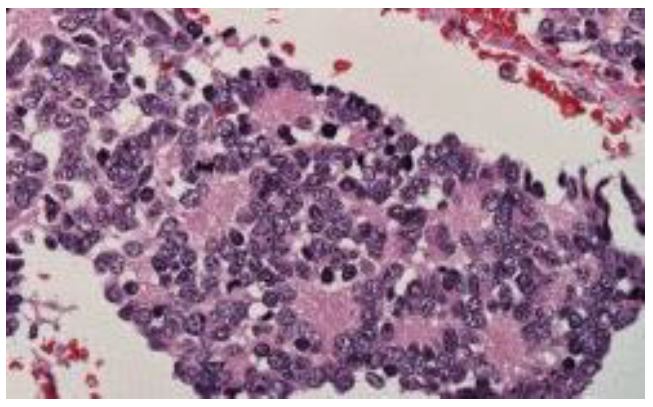
3. Histologicpatterns: a monomorphic sheet ofundifferentiated cells classically noted as small, blue, round cells; presence of Homer Wright rosettes[(菊形團(rosettes)是腫瘤中細胞聚集成一團的構造、他們的中央通常有輻射狀或暈的排列,而命名的由來是哥德式教堂彩色玻璃中的玫瑰花瓣狀,而菊形團(rosettes)具有很多不同的形態,他們的名稱也不進相同; James Homer Wright首次對這種類型的菊形團(rosettes)做命名,常見於Neuroblastoma(神經母細胞瘤)、medulloblastomas(髓母細胞瘤)、primitive neuroectodermal tumors, PNET(原始神經外胚層腫瘤)特色是在腫瘤細胞中央是一塊均質的區域)]
4. S/S: IICP (i.e., headache,nausea, vomiting, mental status changes, and hypertension) andcerebellar dysfunction (i.e., ataxia, poor balance, dysmetria).
5. Standardclinical staging evaluation: MRI of the brain and spine, bothpreoperatively and postoperatively; lumbar puncture after theIICP has resolved.
6. The Chang staging system, originally basedon surgical information, has been modified to incorporate informationfrom neuroimaging to identify risk categories.
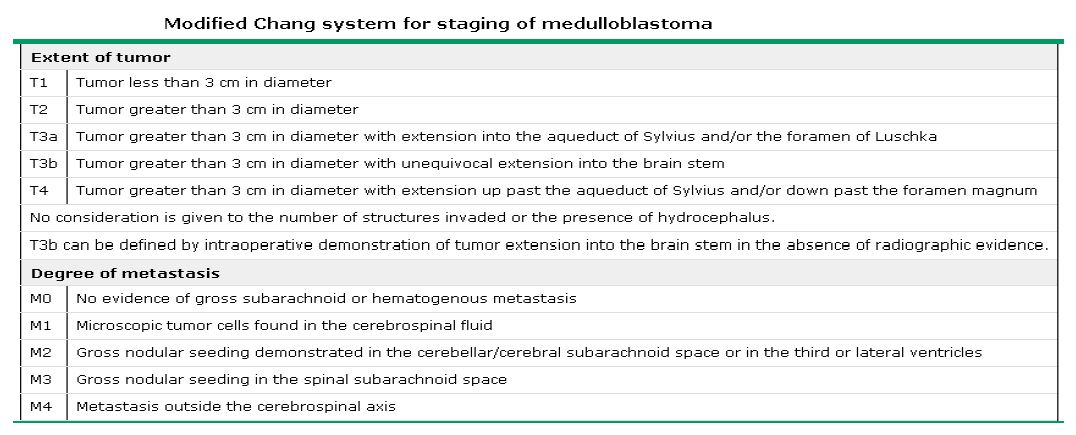
7. Prognostic significance: include age atdiagnosis, extent of disease, and extent of surgical resection; (1) patients younger than 4 yr of age: a poor outcome, partly as the result ofa higher incidence of disseminated disease; (2) patientswith disseminated disease at diagnosis (M >0), including positive CSFcytologic result alone (M1), have a markedly worse outcome than thosepatients with no dissemination (M0); (3) similarly, patients with grossresidual disease after surgery have worse outcomes.
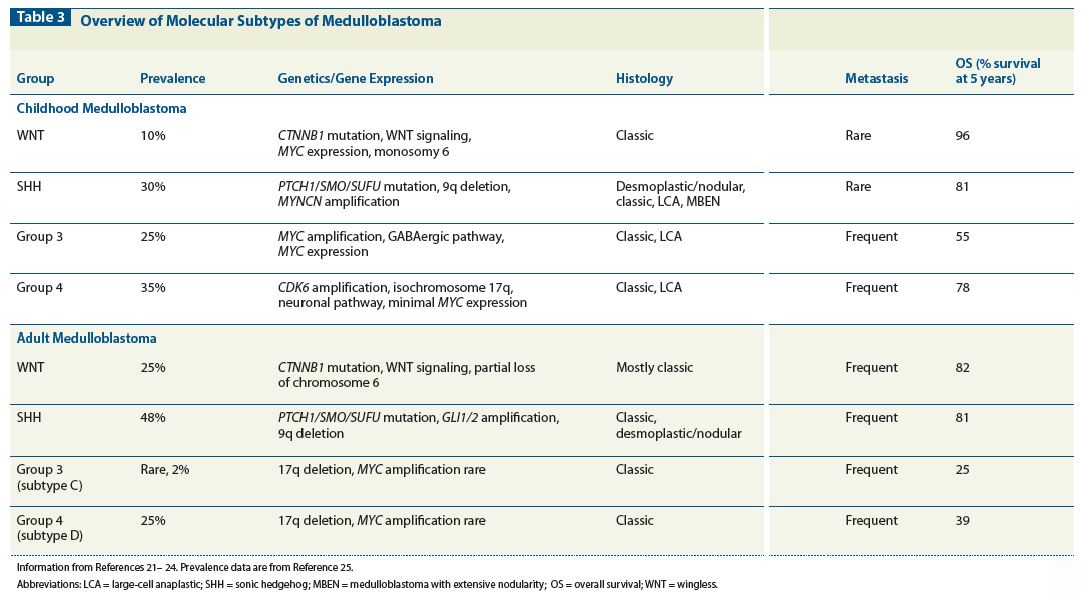
8. Cytogenetic and molecular genetic studies have demonstrated multipleabnormalities in medulloblastoma. The most common abnormalityinvolves chromosome 17p deletions, which occur in 30-40% of allcases. These deletions are not associated with P53 mutations. Severalsignaling pathways have been shown to be active in medulloblastomas, including the sonic hedgehog (SHH) pathway, predominately associatedwith the desmoplastic variants, and the WNT pathway, which canoccur in up to 15% of cases and has been associated with improvedsurvival. Integrative genomic studies have recently identified at least 4 distinct molecular subgroups of medulloblastoma—WNT, SHH, group3, and group 4. These prognostic groups still mustbe validated in larger prospective studies.
9. Treatment: surgery as the starting point of treatment; medulloblastoma issensitive to both chemotherapy and radiation therapy; theoverall outcome approaches 60-70%.
10. Standardradiation treatment in standard risk medulloblastoma incorporatescraniospinal radiation at a total cumulative dose of 24 Gy, with acumulative dose of 50-55 Gy to the tumor bed.
11. Craniospinal radiationat this dose in children younger than 3 yr of age results in severe late neurologic sequelae, including microcephaly, learning disabilities, cognitiveimpairment, neuroendocrine dysfunction (growth failure, hypothyroidism,hypogonadism, and absence/delay of puberty), and/orsecond malignancies.
12. In older children, late sequelae, suchas learning disabilities, neuroendocrine dysfunction, and/or secondmalignancies, can occur.
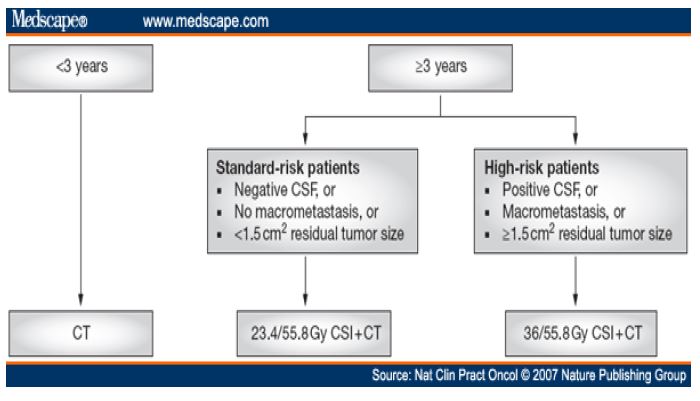
13. These observations have resulted in stratificationof treatment approaches into the following 3 strata: (1) patientsyounger than 3 yr of age; (2) standard-risk patients older than 3 yr of age with surgical total resection and no disease dissemination (M0);and (3) high-risk patients older than 3 yr of age with disease dissemination(M >0) and/or bulky residual disease after surgery.
14. With therisk-based approach to treatment, children with high-risk medulloblastoma receive high-dose cranial–spinal radiation (36 Gy) with chemotherapyduring and after radiation therapy, and those with standard-risk (nonmetastatic) disease receive lower-dose craniospinalradiation (24 Gy) with chemotherapy during and after radiationtherapy.
15. Overall survival in children with nonmetastaticmedulloblastoma andgross total tumor resection approaches 85%. The presence of bulkyresidual tumor (56% survival) or metastases (38% survival) confers apoor prognosis.
2. CT and MRI: a solid, homogeneous,contrast medium–enhancing mass in the posterior fossa causingfourth ventricular obstruction and hydrocephalus; up to 30% of patients with evidenceof leptomeningeal spread.
3. Histologicpatterns: a monomorphic sheet ofundifferentiated cells classically noted as small, blue, round cells; presence of Homer Wright rosettes[(菊形團(rosettes)是腫瘤中細胞聚集成一團的構造、他們的中央通常有輻射狀或暈的排列,而命名的由來是哥德式教堂彩色玻璃中的玫瑰花瓣狀,而菊形團(rosettes)具有很多不同的形態,他們的名稱也不進相同; James Homer Wright首次對這種類型的菊形團(rosettes)做命名,常見於Neuroblastoma(神經母細胞瘤)、medulloblastomas(髓母細胞瘤)、primitive neuroectodermal tumors, PNET(原始神經外胚層腫瘤)特色是在腫瘤細胞中央是一塊均質的區域)]
4. S/S: IICP (i.e., headache,nausea, vomiting, mental status changes, and hypertension) andcerebellar dysfunction (i.e., ataxia, poor balance, dysmetria).
5. Standardclinical staging evaluation: MRI of the brain and spine, bothpreoperatively and postoperatively; lumbar puncture after theIICP has resolved.
6. The Chang staging system, originally basedon surgical information, has been modified to incorporate informationfrom neuroimaging to identify risk categories.
7. Prognostic significance: include age atdiagnosis, extent of disease, and extent of surgical resection; (1) patients younger than 4 yr of age: a poor outcome, partly as the result ofa higher incidence of disseminated disease; (2) patientswith disseminated disease at diagnosis (M >0), including positive CSFcytologic result alone (M1), have a markedly worse outcome than thosepatients with no dissemination (M0); (3) similarly, patients with grossresidual disease after surgery have worse outcomes.
8. Cytogenetic and molecular genetic studies have demonstrated multipleabnormalities in medulloblastoma. The most common abnormalityinvolves chromosome 17p deletions, which occur in 30-40% of allcases. These deletions are not associated with P53 mutations. Severalsignaling pathways have been shown to be active in medulloblastomas, including the sonic hedgehog (SHH) pathway, predominately associatedwith the desmoplastic variants, and the WNT pathway, which canoccur in up to 15% of cases and has been associated with improvedsurvival. Integrative genomic studies have recently identified at least 4 distinct molecular subgroups of medulloblastoma—WNT, SHH, group3, and group 4. These prognostic groups still mustbe validated in larger prospective studies.
9. Treatment: surgery as the starting point of treatment; medulloblastoma issensitive to both chemotherapy and radiation therapy; theoverall outcome approaches 60-70%.
10. Standardradiation treatment in standard risk medulloblastoma incorporatescraniospinal radiation at a total cumulative dose of 24 Gy, with acumulative dose of 50-55 Gy to the tumor bed.
11. Craniospinal radiationat this dose in children younger than 3 yr of age results in severe late neurologic sequelae, including microcephaly, learning disabilities, cognitiveimpairment, neuroendocrine dysfunction (growth failure, hypothyroidism,hypogonadism, and absence/delay of puberty), and/orsecond malignancies.
12. In older children, late sequelae, suchas learning disabilities, neuroendocrine dysfunction, and/or secondmalignancies, can occur.
13. These observations have resulted in stratificationof treatment approaches into the following 3 strata: (1) patientsyounger than 3 yr of age; (2) standard-risk patients older than 3 yr of age with surgical total resection and no disease dissemination (M0);and (3) high-risk patients older than 3 yr of age with disease dissemination(M >0) and/or bulky residual disease after surgery.
14. With therisk-based approach to treatment, children with high-risk medulloblastoma receive high-dose cranial–spinal radiation (36 Gy) with chemotherapyduring and after radiation therapy, and those with standard-risk (nonmetastatic) disease receive lower-dose craniospinalradiation (24 Gy) with chemotherapy during and after radiationtherapy.
15. Overall survival in children with nonmetastaticmedulloblastoma andgross total tumor resection approaches 85%. The presence of bulkyresidual tumor (56% survival) or metastases (38% survival) confers apoor prognosis.