Please click this link for pretest.請點選此連結進行前測。
Chief complaint
chronic productive cough for 3 months
Present illness
This is a 65 y/o man with past history of 1. Ulcerative gastritis s/p panendoscopy s/p PPI since 2018/04/07 and 2. Electrified injury s/p debridement and skin graft 15 years ago.
His ADL was totally independent. Lived in 雲林斗南,occupation: 配電工人, no exposure to fume or exhaust, Smoke: 1.5 PPD for 20 years and quitted for 20 years. While his father was diagnosed with TB and complete treatment for 6 months about 10 years ago.
Since 2017/12, he complaint of persist productive coughing. The sputum was yellow at first and then more whitish recently. No blood tinged. The cough was prominent at night and accompany with sorethroat. There was a bubbling sound at the throat heard when he lay down. The symptom was not relieved with medications prescribed as bronchodilator, antihistamine or anti-tussives. No SOB, DOE, chest tightness, chest pain. Hoarseness voice was noted 2 months ago. Bilateral low back pain will become severe after working or squatting. He had poor appetite and body weight loss from 50 to 45 kg in 3 monhths. In OPD, CXR revealed bilateral upper field increased infiltration.
Under impression of pnuemonia, r/o TB, r/o lung CA, he was admitted for further evaluations and management.
Figure 1. CXR image at OPD:
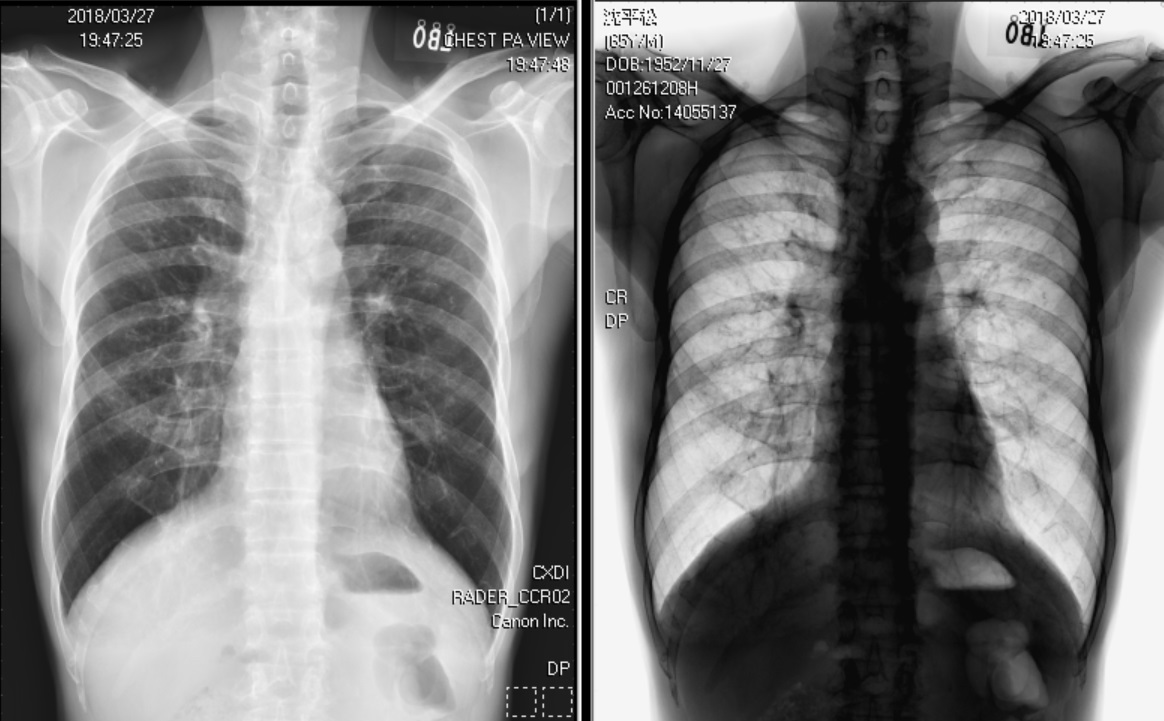
Normal chest X-ray and inverted chest X-ray.
Past history and Past psychiatric history:
過去精神病史: Denied
DM: No
HTN: No
Hepatitis: No
Operation:
Electrified injury s/p debridement and skin graft 15 years ago.
Personal History
Smoking: 1.5 PPD for 20 year(s), quit for 20 year(s)
Alcohol: wine: 40-50%, amount: 30mL for 40 year(s), quit or not : no.
Betel nuts: 20 years. Quit now
Travel history
No
Allergy history
Drug : Nil
Food : Nil
Blood transfusion : Nil
Family history
Significant disease history in the family: Nil
Contact History
No
Physical Examination
Chest:
Inspection: Normal and symmetric respiratory movement , No deformity , Normal breast
Palpation: No palpable mass , No tender point , No vocal fremitus , No subcutaneous crepitance
Auscultation: No rales , No rhonchi , No wheezing
Laboratory Data
GOT/GPT/TB 42/27/(107/4/9);
WBC/HGB/PLT 5750/14.6/238k(107/4/9);
BUN/Cr /0.97(107/4/9);
LDH/Ca 372/8.7(107/4/9);
Figure 2. Chest CT image

Diffuse emphysema of both lungs with focal bronchiectasis and bronchial wall thickening is mentioned with peribronchial infiltrates and small peribronchial nodules(more obvious in RUL and LUL). The possibility of COPD with chronic bronchiolitis is more likely than lung to lung metastasis.
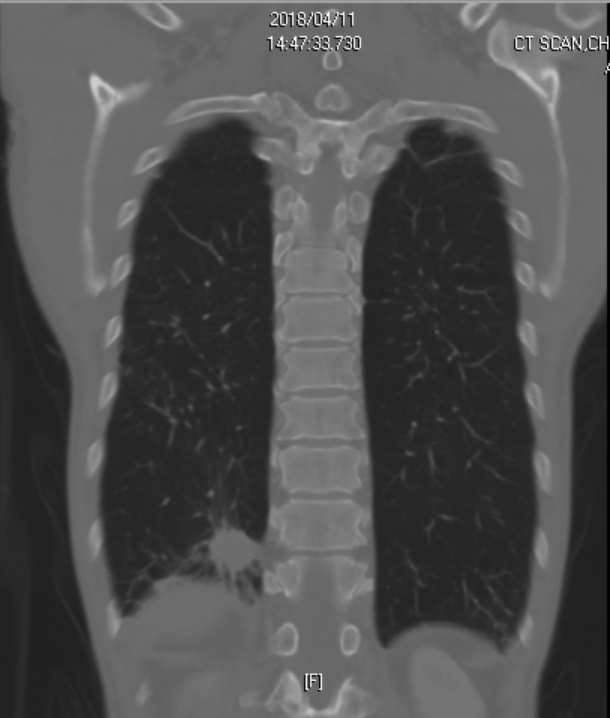
A solid mass 3cm is located in basal segment of RLL of lung with pleural retraction. Lung cancer can not be ruled out.
Figure 3. PFT
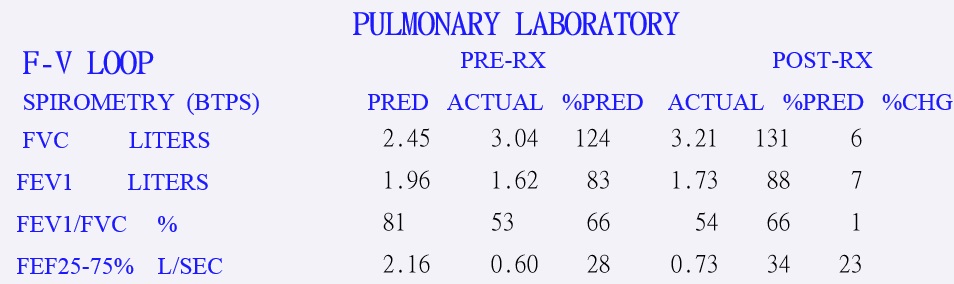
Moderately obstructive ventilatory impairment.Negative bronchodilator response.
 2022/9/14 8:09:54
2022/9/14 8:09:54
 887
887


